


Abortion 'Stigma' Concerns Health Ministry
The five-year review of Jacinda Ardern’s radical extreme abortion law which opened the door to late term abortions was quietly released by the Ministry of Health last month. It's depressing.

In the dark of the night last month, the Ministry of Health released a report – but didn’t tell anyone.
It was the five year review following Jacinda Ardern’s radical extreme abortion law which opened the door to late term abortions – even though the proponents of the radical law will deny that – but this latest review does, and has a whole section on it.
Now if the Ministry was lobbying for liberal abortion laws and there were still restrictions on abortion, then the media would have been all over this report – and this issue in general.
But because we now have one of the most liberal abortion laws in the world and late term abortions are available with a wink and a nod from two abortionists, then the media have moved on. Nothing to see here.
Its quite a contrast isn’t it. It’s only when abortion may be under threat that the media are remotely interested in it.
But this new report still makes sickening reading – and should make you question anything which comes out of the Ministry of Health.
Titled Review of Certain Matters under the Contraception, Sterilisation, and Abortion Act 1977, the introduction says
On 24 March 2020, changes were made to the law to decriminalise abortion… Since 2020 the Ministry of Health has worked towards achieving these changes through focusing on…
And one of the categories is
services that are more person-centred
Just not the person in the womb.
But the Ministry is very pleased with its performance, saying:
Overall, access to abortion services has increased since the law change… This is a positive sign that those seeking care are experiencing fewer barriers and that the initiatives to improve access, like self-referral and telehealth, are making an impact.
Note the terminology – those seeking “care”. And of course “access” equals more abortions.
You quickly get a warped worldview from the authors of this report just by the Glossary of Terms at the beginning.
They don’t define “man” or “men”, but they do tell you what a “woman” is! Unfortunately they got the definition from either Chris Hipkins or the Midwifery Council.
In line with the Women’s Health Strategy (2023) it is recognised that not everyone who experiences the health issues covered in this report [i.e. pregnancy] are women. The contraception, sterilisation, and abortion health care needs discussed in this report can be experienced by people with diverse gender identities and expressions and sex characteristics. It is intended that the recommendations within this report will be inclusive of rainbow voices and work to drive services and approaches that respond to rainbow needs and aspirations.
So they do use that highly offensive word “woman” – but they don’t really mean it.
Now to push their narrative, the Ministry commissioned three research groups. Nope – not trad mums, or religious conservatives, or wives. Don’t be silly.
There is a research report on 124 wahine focusing on aborting more unborn Maori and Pacifika children. A research report focusing on how disabled people should have better access to abortions – no mention of the disabilities of the unborn child of course. And a research report of 10 LGBTQ+ people who needed an abortion, co-authored by none other than ex-Green MP Elizabeth Kerekere who was expelled from the Greens for allegations of bullying.
I’ll come back to that paper because you’re probably asking right now – how do same sex couples get pregnant? Good question.
So let’s just check out some of the narrative of this report – which is basically saying that abortion access has increased, abortions have increased, but how can we enable more.
It’s actually quite sickening.
The first red flag is in the area of counselling.
Between 2022 and 2024, we observed a 35% decrease in women accessing pre-abortion counselling, despite a 21% increase in the total number of abortion procedures provided over this same period.
You can see it in this graph this decrease – and this is concerning. How much thought has the pregnant woman put into what will be a life-changing event. And do they know the better options?
But the law only requires women to know about abortion – not to have to receive counselling.
As I mentioned earlier, this research paper doesn’t hide the fact that late term abortions are happening i.e. 20 weeks onwards
Here’s where surgical abortions are happening – primarily in hospitals – but surgical is decreasing as medical (taking medication to kill the unborn child) is increasing. But note the key on the right – 20 weeks, over 20 weeks.
And you can see the big growth in medical abortions – that’s the blue line – because apparently medical abortions are a great option, except they’re not.
A study released a couple of weeks ago found that more than 1 in 10 women who take the abortion pill mifepristone to complete a chemical abortion will suffer a serious health complication during the process.
The study of 865,727 patients between 2017 and 2023, which was published by the Ethics and Public Policy Center (EPPC) discovered that 11% of women suffer at least one “serious adverse event” within 45 days of taking mifepristone for an abortion. More than 4.7% were forced to visit an emergency room related to the abortion, more than 3.3% suffered hemorrhaging, and more than 1.3% got an infection. Thousands were hospitalized, more than 1,000 needed blood transfusions, and hundreds suffered from sepsis. Nearly 2,000 had a different life-threatening adverse event.
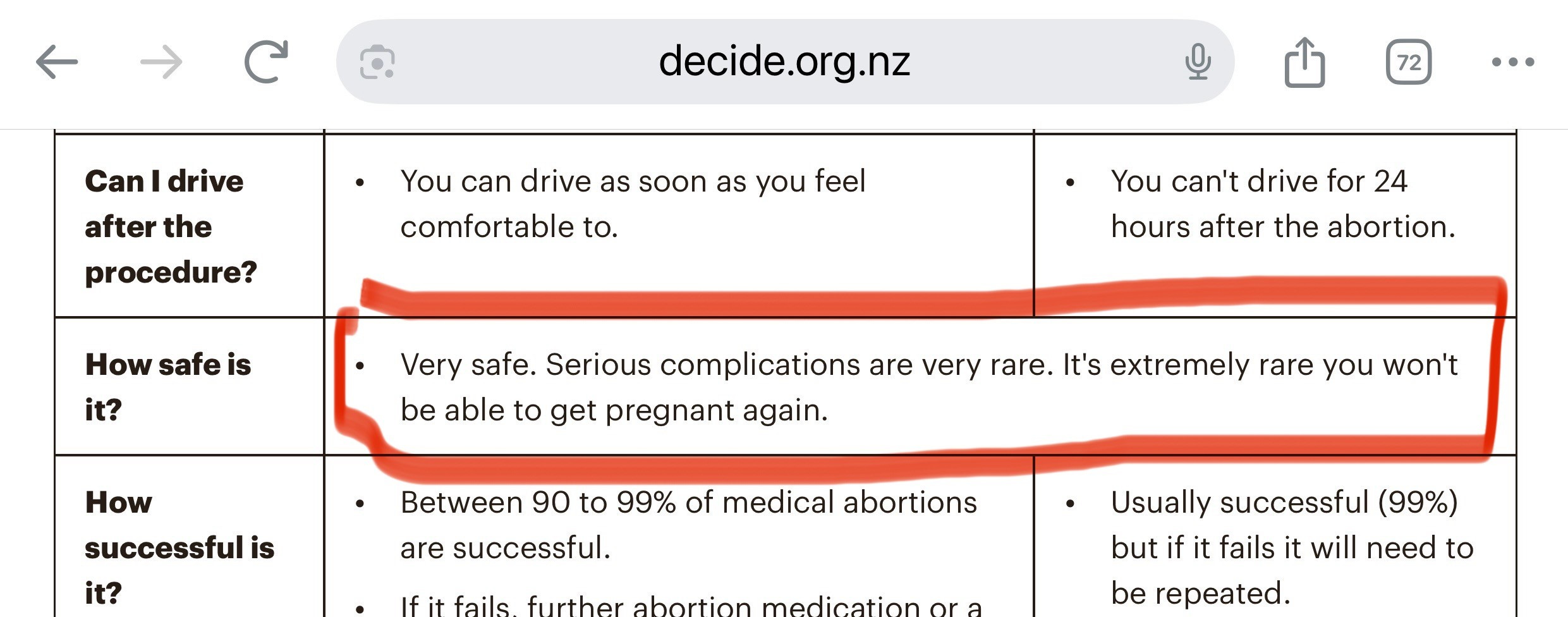
But look at what the Ministry of Health tells women. Very safe.
Very safe – except for the 1 in 10 women who will have a serious adverse event.
So much for informed consent eh.
There is then a section on “Later surgical abortion”.
“13 to 26 weeks”
Yep, 2nd trimester – but post-20 weeks. Previously, the Crimes Act allowed for an abortion after 20 weeks’ gestation only in exceptional circumstances. The new law means that a woman can have a late-term abortion if the abortion provider in consultation with another abortion provider ‘reasonably believes the abortion is clinically appropriate in all the circumstances,’ having regard to the woman’s physical and mental health and wellbeing. This is a very broad, subjective test. The terms ‘physical health’, ‘mental health’ and ‘wellbeing’ are not defined by the law. The gestational age to be considered is not defined.
In fact, official statistics shows that between 2021 and 2023, there was a 67% increase in late term abortions.
Note the language of this paper. “Later surgical abortion” – but of course they’re referring to late term abortions. They just don’t like saying it.
And just to reiterate – a section on late term abortion “care”
But they appease their conscience by suggesting that it’s only 1% of abortions – but admit that post-22 weeks, it’s a “significant challenge” because most medical professionals are pro-life and want nothing to do with killing an unborn child.
Which is why the workforce is so small. I’ll come back to that in just a second.
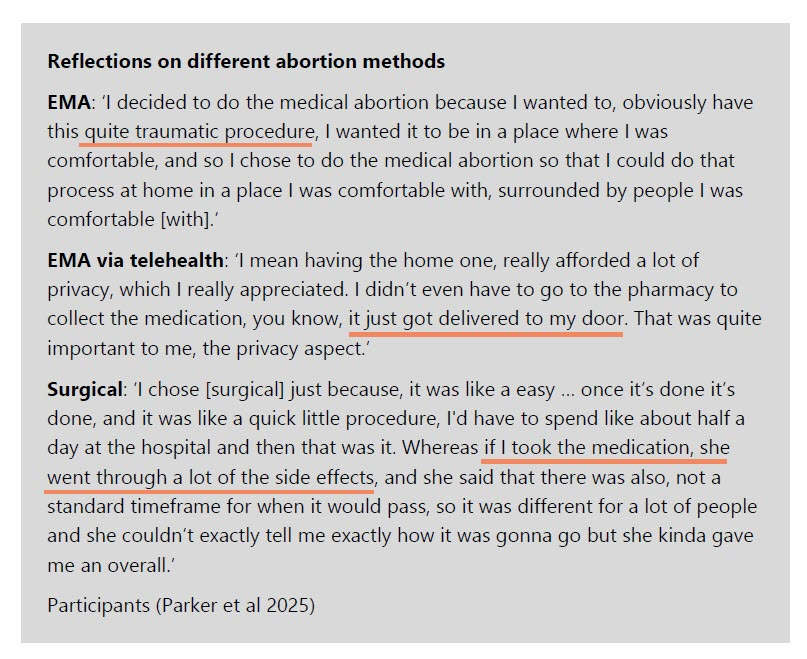
But note this part of the report. It’s a couple of testimonies from women who have had abortions using different abortion methods – EMA = early medical abortion.
I think they said the quiet parts out loud:
…this quite traumatic procedure
…I didn’t even have to go to the pharmacy to collect the medication, you know, it just got delivered to my door.
…if I took the medication, she went through a lot of the side effects, and she said that there was also, not a standard timeframe for when it would pass,
Traumatic. Side effects. Just get it couriered – too bad if there’s complications.
Now one of the most positive aspects of this report – if you can call it positive – is that the abortion workforce is tiny in NZ.
And the Ministry of Health is concerned about this.
The size of the abortion workforce has increased over the last five years. However, the number of practitioners providing abortion services is still a small proportion of the wider workforce of registered doctors, midwives and nurses.
Excellent.
In 2021, the Ministry ran a procurement process to support practitioners in providing abortion in primary care… developed a training programme with the aim of increasing primary care provision of abortion services…. From November 2022 when training was launched until 30 October 2024, 214 health practitioners have completed the modules. The Ministry does not hold data on how many of these practitioners have since provided abortion services.
Now to put that in perspective, there are 17,000 doctors in NZ and 58,000 nurses. So that abortion workforce represents 0.4% of the workforce. 99.6% of medical professionals want nothing to do with killing the unborn babies.
In fact, the paper also refers to another research report – this one - “Willing but not able: A survey of New Zealand health practitioners' interests in providing second trimester abortion care and the obstacles they face.”
The researchers wanted to survey health practitioners about doing second trimester abortions.
They canvassed far and wide
Recruitment was via an exponential non-discriminating snowball email survey sent to members of abortion Providers of Aotearoa New Zealand, Clinical Directors of each District Health Board (DHB), New Zealand Midwifery Council and hospital obstetrics and gynaecology (O&G) department clinical directors. The electronic survey link was also published by The Royal College of General Practitioners of New Zealand newsletter, ePulse, and on the Facebook group NZ Women in Medicine. Those who received the survey were asked to forward it to other health practitioners with a possible interest in abortion care.
That’s a massive pool. Guess how many respondents they got to this anonymous electronic survey.
113.
Yep. 113.
You might remember The Spinoff whining a couple of years ago about Middlemore hospital struggling to find staff to perform abortions. Isn’t that great!
Because of the unwillingness of medical professionals to take life, the report also touches on conscientious objection, and says
The Ministry of Health is aware of some reports that conscientious objection plays a part in the decision by some health care providers not to provide abortion care… Failure to reduce the impact of conscientious objection on abortion service provision contributes towards the overall inequity in accessing abortion services around the country.
This is code for – we may need to force some places and people to have to provide abortions.
How do they do that?
There is the potential for an employer to terminate a position, or to refuse to hire someone, on the grounds of his or her conscientious objection. Sadly, at the time of passing the new abortion law in 2020, a majority of MPs voted against proposed amendments to keep conscientious objection standards the same as they were under the previous law.
The paper says
one member commented ‘entire hospitals have claimed to be conscientious objectors, leading to wide disparities in access to care’.
No – that is care. Care for the pregnant woman. Care for the life of the child. That sounds like a good hospital to both work at and be a patient at. They understand the sanctity of life. All life.
Just finally, the report is concerned about Abortion Stigma.
one of the changes to abortion law in 2020 was to remove abortion care from the Crimes Act 1961 and recognise it instead as a health care service. From the consumer research we commissioned, it appears that while this change has helped to reframe how society views abortion health care, stigma surrounding abortion remains. For some patients, the stigma can still have an impact on their decision-making and their access to abortion care… many participants found abortion was ‘emotionally complex’. Some felt that in deciding to have an abortion they were doing something wrong.
Does this surprise you?
The stigma is a healthy stigma. The new law has given the unborn baby the same status as an appendix, gall bladder or tonsils – simply ’tissue’ removed as part of a ‘health procedure’. But anyone who has viewed the ultrasound of an unborn child will know that this is a gross abuse of human rights.
The Ministry paper offers no solution to this.
That’s because the solution of removing the stigma goes against the complete narrative of this awful document.
Interestingly, the paper mentions a little further on, it says
From its research, National Centre for Women’s Health Research Aotearoa found that having an ultrasound before the appointment at the abortion service presented a considerable time and cost barrier to wāhine.
The cost issue is a big fat smokescreen.
Research suggests that seeing a baby on ultrasound during pregnancy can have positive maternal psychological effects, potentially reducing anxiety and fostering a stronger bond with the fetus.
Pro-abortion advocates don’t like women seeing ultrasounds – because it reinforces the humanity of the unborn child, and completely destroys the false narrative that this is just a blob of tissue or a clump of cells.
Finally (!) there is a section on sex selection.
This is pretty shocking eh. I mean – biological sex selection. Almost as though the baby is born male or female. How binary. I’m not sure how that got past the woke police.
Anyways – it says
During the Select Committee process in 2019, committee members were concerned about estimates from the UNFPA about the number of women missing due to gender-biased sex selection through abortion. Members recognised that there was no evidence of this occurring in New Zealand
Of course they don’t say how they know there is no evidence – or how they actually checked.
Hint – they didn’t check.
Sex selective abortion is a well-known problem in China and India, where son-preference cultures have resulted in extremely skewed sex ratios. There is evidence that sex-selective abortion is already occurring in other countries, including Canada and Australia.
In New Zealand, a majority of MPs voted against a proposed amendment to explicitly outlaw sex-selective abortions. It begs the question - what were they scared of by having the law? What were they trying to hide?
It continues
While the Select Committee considered options for responding using legislation or other means, most members agreed that setting a restriction through legislation could lead to ethnic profiling, women not disclosing about sex selection or women seeking unlawful abortions. As a result of Select Committee considerations and feedback on this issue, section 21 of the CSA Act now states that Parliament opposes the performance of abortions being solely sought because of the preference for the fetus to be of a particular sex.
Once again, not a shred of evidence – and no specific law to enforce what Parliament thinks.
All bull and bluster.
The paper then admits that a woman seeking an abortion at earlier than 20 weeks’ gestation does not need to give a reason – so they have no data on sex selection anyway.
Yet in the 2023 abortion statistics report, it noted that six abortion places had acknowledged that sex selection abortions were a reason or possibly a reason for requesting an abortion – but
neither the CSA Act nor any associated legislation gives any direction on what actions would arise from such a notification, and the Ministry does not have internal processes for responding to one.
Head in the sand eh.
Before I go, let’s just check that research report of 10 LGBTQ+ people who needed an abortion, co-authored by none other than ex-Green MP Elizabeth Kerekere who was expelled from the Greens for allegations of bullying, and a few others including a non-binary Pakeha health researcher
This is the cover. Obviously the budget for a graphic designer wasn’t that high.
But let me just read you a few sections of this report of 10 LGBTQ+ people who needed an abortion – in other words, biological females who needed an abortion because they were pregnant – which only females can become pregnant.
Here’s a few classic bits
The majority of the research that considers experiences of abortion does so from a cis-heteronormative lens, meaning that service users are assumed by default to be cisgender and heterosexual and little or no attention is given to the genders or sexualities of service users.
False. It’s all females. Sexuality is actually irrelevant. If they’re pregnant, it was with a male.
It’s really quite easy, isn’t it.
Bisexual cisgender women may also engage in sexual behaviours at a younger age than heterosexual and lesbian cisgender women… Consequently, bisexual cisgender women were found to be up to three times as likely as heterosexual cisgender women to have had an abortion
Yes one of the sad observations about young people who are both sexually and gender confused is that they are much more likely to be sexually active and also using drugs.
Sadly – and to add to the negative outcomes – they may think abortion is the answer. It’s not.
Abortion care delivered on the assumption that service users are cisgender women results in the invisibility of transgender and non-binary people in abortion services
No – nothing to do with “invisibility”. We see you. It’s just that only women can get pregnant. It’s a biological thing. You’ll be recognised as a female, because blokes like me can’t get pregnant.
The “assumption” is medically based – and reality based.
And then who were the subjects in this so-called credible report relied on by the Ministry of Health?
Eight participants were cisgender women, one was a transman, and one was non-binary. No participants were intersex. Eight participants were bisexual and/or pansexual, and two were queer.
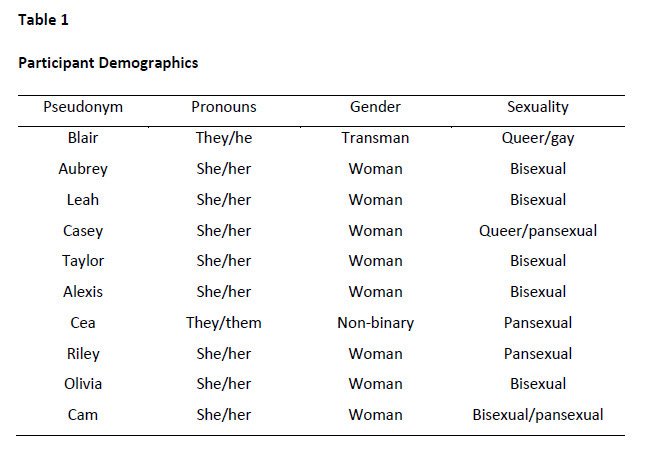
Here’s the make-up as a grid. Yes – they are serious.
I don’t want to be a smarty-pants – and I’m not a biologist - but that means there were 10 females. You can put any label you want on it – trans, cis, non-binary – but it’s still 10 women – adult human females – who can get pregnant. And ironically, it will have involved a male somewhere in the process.
Biology 101.
Did the report have any limitations (apart from the authors and the pre-conceived ideologies, of course!)?
While the current research engaged a diverse sample, a limitation is the small number of trans and non-binary people who participated in interviews. It is, however, possible that this silence is reflective of the erasure that trans and non-binary people face in sexual and reproductive health services more generally.
Silent, erasure, invisibility. Lots of gaslighting words there.
The problem is that abortion is about a pregnant female killing the unborn child in their womb. End of.
In conclusion, here’s the problem.
As well as commissioning an ideologically confused report on bisexual cisgender women and transmen, this Ministry of Health report takes a dangerous flawed and non-health approach.
It’s unapologetically pro-abortion.
It celebrates more abortion – not less
It refuses to acknowledge the risks and harms to the women.
It makes no recognition of the unborn child – despite other health messages which encourage women to consider the health of the unborn child such as drug use, alcohol use during pregnancy etc
There is no consideration of the benefits of reducing abortions
This research report is an obituary to the deaths of 16,000+ babies in the womb every year, and thousands of women (and men) who will be forever harmed by abortion.
We do not have a Ministry of Health. It’s a Ministry of Ideas. Dangerous ideas.
Treat them with the contempt they deserve.
As usual I have mixed feelings about your article Bob. You are obviously passionate about the topic, and with good reason. I am with you 100% about the ridiculous sophistry that gender 'academics ' like Elizabeth Kerekere profess as science. You can't outrun biology no matter what their spurious social engineering propaganda says.
As far as termination goes, as a man, I feel uneasy about lecturing women about what they choose to do their body.
I will say that I don't think abortion should be used as a contraceptive. If a woman is sexually active and doesn't want children then there are better options. I also think 20 weeks and beyond is in general too late to choose,17 or 18 weeks is more than enough time to make a rational decision. Obviously if the case of rape,incest or significant foetal abnormalities there could be some flexibility.
I certainly don't want to live in some patriarchy driven Handmaid's Tale dystopia. It's telling when prolife activists are also proponents of harsh prison sentences. The children of unwanted pregnancies often end up in our courts and prisons. The interest of pro-lifers in a baby nearly always ends at birth.
Just a thought.
Andrew McKenna